| Leiomyosarcoma | |
|---|---|
| Other names: LMS | |
 | |
| Leiomyosarcoma of the adrenal vein. Coronal view of abdominal MRI. Tumor (arrow) extends from the superior pole of the right kidney to the right atrium. | |
| Specialty | Hematology and Oncology |
Leiomyosarcoma is a cancerous smooth muscle tumor.[1]
A benign tumor originating from the same tissue is termed leiomyoma. While leiomyosarcomas are not thought to arise from leiomyomas,[2] some leiomyoma variants' classification is evolving.[citation needed]
About one in 100,000 people get diagnosed with leiomyosarcoma (LMS) each year.[3] LMS is one of the more common types of soft-tissue sarcoma, representing 10 to 20% of new cases. (Leiomyosarcoma of the bone is more rare.) Sarcoma is rare, consisting of only 1% of cancer cases in adults.[4] Leiomyosarcomas can be very unpredictable; they can remain dormant for long periods of time and recur after years. It is a resistant cancer, meaning generally not very responsive to chemotherapy or radiation. The best outcomes occur when it can be removed surgically with wide margins early, while small and still in situ.[5]
Signs and symptoms[edit | edit source]
The clinical presentation of this condition is consistent with:[6]
- Fatigue
- Fever
- Nausea
- Weight loss
Mechanism[edit | edit source]
Smooth muscle cells make up the involuntary muscles, which are found in most parts of the body, including the uterus, stomach and intestines, the walls of all blood vessels, and the skin, so leiomyosarcomas can appear at any site in the body. They are most commonly found in the uterus,[7] stomach,[8] small intestine and retroperitoneum.[9]
Uterine leiomyosarcomas come from the smooth muscle in the muscle layer of the uterus.[10] Cutaneous leiomyosarcomas derive from the pilo-erector muscles in the skin. Gastrointestinal leiomyosarcomas might come from smooth muscle in the GI tract, or alternatively, from a blood vessel. At most other primary sites—retroperitoneal extremity (in the abdomen, behind the intestines), truncal, abdominal organs, etc.—leiomyosarcomas appear to grow from the muscle layer of a blood vessel (the tunica media). Thus, a leiomyosarcoma can have a primary site of origin anywhere in the body from a blood vessel.[5]
The tumors are usually hemorrhagic and soft and microscopically marked by pleomorphism, abundant (15–30 per 10 high-power fields) abnormal mitotic figures, and coagulative tumor cell necrosis. The differential diagnosis, which includes spindle cell carcinoma, spindle cell melanoma, fibrosarcoma, malignant peripheral nerve sheath tumor and even biphenotypic sinonasal sarcoma, is wide.
Diagnosis[edit | edit source]
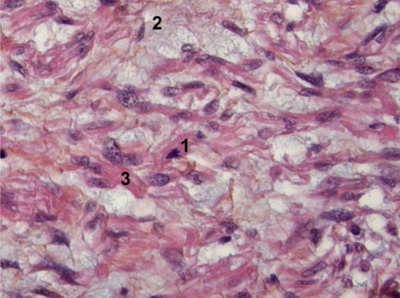
Myxoid leiomyosarcoma of bladder- 1) Abnormal mitosis 2) differentiated leiomyosarcoma 3) pools of hyaluronic acid
![Histopathology of leiomyosarcoma shows variable atypia, often with cytoplasmic vacuoles at both ends of nuclei, and frequent mitoses.[11]](data/media/images/398px-Histopathology_of_leiomyosarcoma.jpg)
Histopathology of leiomyosarcoma shows variable atypia, often with cytoplasmic vacuoles at both ends of nuclei, and frequent mitoses.[11]

![Histopathology of leiomyosarcoma shows variable atypia, often with cytoplasmic vacuoles at both ends of nuclei, and frequent mitoses.[11]](https://mdwiki.org/wiki/https://mdwiki.org/wiki/File:Histopathology_of_leiomyosarcoma.jpg)
Diagnosis of LMS is made by performing a soft-tissue biopsy and examining its histopathology.[medical citation needed]
Treatment[edit | edit source]
Surgery, with as wide a margin of removal as possible, has generally been the most effective and preferred way to attack LMS. If surgical margins are narrow or not clear of tumor, however, or in some situations where tumor cells were left behind, chemotherapy or radiation has been shown to give a clear survival benefit.[12] While LMS tends to be resistant to radiation and chemotherapy, each case is different and results can vary widely.
For metastatic (widespread) disease, chemotherapy and targeted therapies are the first choices. Chemotherapy regimens are include: doxorubicin/ ifosfamide and doxorubicin combination/gemcitabine and docetaxel/ trabectedin;[13] pazopanib is the targeted therapy used in metastatic leiomyosarcoma as second line and is well tolerated.[14]
LMS of uterine origin often responds to hormonal treatments.[15][16] As of 2020, several clinical trials for uterine LMS are active.[17]
Notable cases[edit | edit source]
People who have had leiomyosarcoma include:
- Leicester City footballer Keith Weller, who made over 300 appearances for the Foxes, scored 47 goals. Also, he made four appearances for England, scoring one goal.[18]
- Katie Price[19]
- Canadian public-health physician Sheela Basrur (1956–2008) developed uterine leiomyosarcoma in 2006.[20]
- American actress Diana Sands[21]
- Canadian comedian Irwin Barker was featured in a documentary, That's My Time, which chronicled his battle with leiomyosarcoma.[22]
- E. J. McGuire, long-time professional ice hockey coach, scout, and vice president of the National Hockey League Central Scouting Bureau[citation needed]
- Ellis Avery, American writer, two-time winner of the Stonewall Book Award[citation needed]
See also[edit | edit source]
References[edit | edit source]
- ↑ WHO Classification of Tumours Editorial Board, ed. (2020). "1. Soft tissue tumours: Smooth muscle tumours - Leiomyosarcoma". Soft Tissue and Bone Tumours: WHO Classification of Tumours. Vol. 3 (5th ed.). Lyon (France): International Agency for Research on Cancer. pp. 195–197. ISBN 978-92-832-4503-2. Archived from the original on 2021-06-13. Retrieved 2022-06-25.
- ↑ Kumar, Vinay; Abbas, Abul; Aster, Jon (2015). Robbins and Cotran Pathologic Basis of Disease. Philadelphia, PA: Elsevier. pp. 1020–1021. ISBN 978-1-4557-2613-4.
- ↑ "Surveillance, Epidemiology, and End Results (SEER) Program Stat Database: Incidence—SEER 18 Regs Research Data + Hurricane Katrina Impacted Louisiana Cases, Nov 2016 Sub 2000-2014 Katrina/Rita Population Adjustment—Linked To County Attributes - Total U.S., 1969–2015 Counties, DCCPS, Surveillance Research Program". National Cancer Institute. April 2017. Archived from the original on April 30, 2019. Retrieved June 6, 2017.
- ↑ Serrano, Cesar; George, Suzanne (2013). "Leiomyosarcoma". Hematology/Oncology Clinics of North America. 27 (5): 957–74. doi:10.1016/j.hoc.2013.07.002. PMID 24093170.
- ↑ 5.0 5.1 "Basic info". Leiomyosarcoma.info. Archived from the original on 2009-04-30.
- ↑ "Leiomyosarcoma". NORD (National Organization for Rare Disorders). Archived from the original on 22 January 2022. Retrieved 25 January 2022.
- ↑ Arnold LM, Burman SD, O-Yurvati AH (April 2010). "Diagnosis and management of primary pulmonary leiomyosarcoma". J Am Osteopath Assoc. 110 (4): 244–6. PMID 20430913. Archived from the original on 2019-02-09. Retrieved 2021-04-25.
- ↑ Mehta, Varshil; Rajawat, Monali; Rastogi, Sameer; Phulware, Ravi H; Mezencev, Roman (2017-11-21). "Leiomyosarcoma of the stomach with metastasis to the liver: a case report with review of the literature". Future Science OA. 4 (2): FSO264. doi:10.4155/fsoa-2017-0100. PMC 5778386. PMID 29379638.
- ↑ Piovanello P, Viola V, Costa G, et al. (2007). "Locally advanced leiomyosarcoma of the spleen. A case report and review of the literature". World J Surg Oncol. 5 (1): 135. doi:10.1186/1477-7819-5-135. PMC 2221972. PMID 18045454.
- ↑ Sue Ghosh; Jonathan Hecht; Tanaz Ferzandi; Christopher Awtrey (2007). "Leiomyosarcoma of the Uterus (ULMS): A Review". The Liddy Shriver Sarcoma Initiative. Archived from the original on 15 June 2012. Retrieved 1 February 2016.
- ↑ Vijay Shankar, M.D. "Soft tissue - Smooth muscle - Leiomyosarcoma - general". Pathology Outlines. Archived from the original on 2021-04-13. Retrieved 2021-04-25. Topic Completed: 1 November 2012. Revised: 11 September 2019
- ↑ "About Chemotherapy". Leiomyosarcoma.info. August 2002. Archived from the original on 2009-06-25.
- ↑ Rastogi, Sameer; Bakhshi, Sameer (2016). "Trabectedin in Soft Tissue Sarcoma: Have We Hit the Bull's-eye?". Journal of Clinical Oncology. 34 (29): 3582–3583. doi:10.1200/jco.2015.65.7130. PMID 27458287.
- ↑ Rastogi, Sameer; Sharma, Aparna; Vanidassane, Ilavarasi; Aggarwal, Aditi; Mridha, Asitranjan; Pandey, Rambha; Dhamija, Ekta; Barwad, Adarsh (2019). "Pazopanib efficacy and toxicity in a metastatic sarcoma cohort: Are Indian patients different?". Indian Journal of Cancer. 56 (3): 207–210. doi:10.4103/ijc.IJC_105_18. PMID 31389382. S2CID 198168573.
- ↑ Abu-Rustum, N. R.; Curtin, J. P.; Burt, M.; Jones, W. B. (1997). "Regression of uterine low-grade smooth-muscle tumors metastatic to the lung after oophorectomy". Obstetrics and Gynecology. 89 (5 Pt 2): 850–852. doi:10.1016/S0029-7844(97)00033-1. PMID 9166348. S2CID 23049718.
- ↑ Hardman, M. P.; Roman, J. J.; Burnett, A. F.; Santin, A. D. (2007). "Metastatic Uterine Leiomyosarcoma Regression Using an Aromatase Inhibitor". Obstetrics & Gynecology. 110 (2 Pt 2): 518–520. doi:10.1097/01.AOG.0000267533.56546.c2. PMID 17666649. S2CID 24257210.
- ↑ "Uterine Sarcoma Clinical Trials". National Cancer Institute. Archived from the original on 2021-05-16. Retrieved 2021-04-25.
- ↑ "Leicester legend Weller mourned". BBC Online. 2004-11-13. Archived from the original on 2008-03-29. Retrieved 2010-05-14.
- ↑ "Jordan treated for cancer". BBC Online. 2002-08-11. Archived from the original on 2009-03-27. Retrieved 2009-10-30.
- ↑ Gillespie, Kerry (2008-04-12). "'Can't ever give up hope,' Basrur says". The Toronto Star. Archived from the original on 2012-10-05. Retrieved 2010-01-08.
- ↑ Brown, Stacia. "Diana Sands: What Was and What Could've Been". Archived from the original on 6 December 2017. Retrieved 25 May 2017.
- ↑ "That's My Time". Irwinbarker.com. Archived from the original on 2008-10-02. Retrieved 5 March 2015.
In Irwin's own words: “Cancer has my body but not my spirit, and I'll continue to make jokes, not so much about cancer, but in spite of it.”
External links[edit | edit source]
| Classification | |
|---|---|
| External resources |